|
|
Mediastinal Teratoma
General Considerations
-
Mediastinum is a rare site for occurrence of teratomas, most being ovarian in origin
-
Arise from primitive germ cell rests
-
May be solid or cystic
-
Three major categories
-
Mature teratomas
-
Well-delineated from surrounding tissues
-
Contain ectodermal elements along with cartilage, fat and smooth muscle
-
Immature teratomas
-
Teratomas with malignant transformation
-
Overall about 30% are malignant
-
Usually adenocarcinoma in mature teratomas
-
Angiosarcoma or rhabdomyosarcoma in immature teratoma
-
Most of the cystic lesions are benign and most of the solid lesions are malignant
-
Both occur early in life—young adults most commonly
-
DDX from thymomas which usually occur in 5th or 6th decade 
Clinical Findings
Differential Diagnosis
Anterior Mediastinal Masses |
|
|
|
|
Associations
- Non-lymphocytic leukemia and malignant histiocytosis with immature teratomas
Imaging findings
-
Most occur in the anterior mediastinum, near junction of great vessels and heart
-
Benign lesions are usually smooth in contour whereas malignant masses tend to be lobulated
-
Usually larger than thymomas
-
Calcification may rarely occur but is of no help since thymomas also calcify
-
CT shows fatty mass with globular calcifications and rarely a tooth or bone
-
Rapid increase in size may mean hemorrhage into a cyst rather than enlarging malignancy
Treatment and prognosis
Other germ cell neoplasms
Mediastinal seminomas
-
Rare
-
Almost always in young men
-
Identical to testicular seminoma and ovarian dysgerminoma
-
May be well-encapsulated or invasive
-
Tends to be lobulated
-
Cannot be differentiated from teratoma
Primary choriocarcinoma
-
Even rarer than seminoma in the mediastinum
-
Only 23 reported in the literature, almost all in men
-
Occur between 20-30 years
-
May be lobulated
-
May have elevated beta sub unit of HCG
-
Growth is very rapid leading to dyspnea, hemoptysis, stridor
-
Gynecomastia and a + Aschheim-Zondek test can occur
-
Rapidly fatal

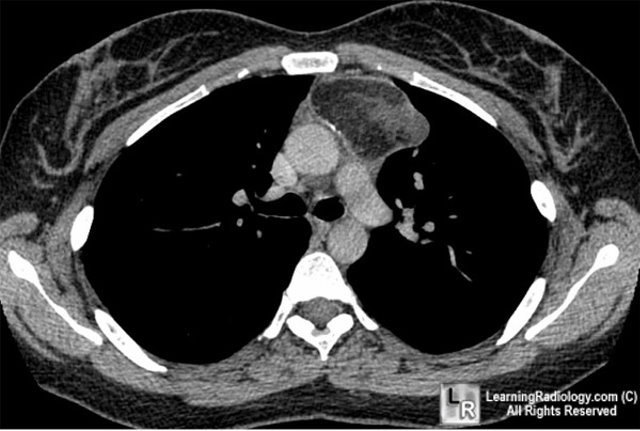
Mediastinal Teratoma. Contrast-enhanced axial CT scan of the chest demonstrates an anterior mediastinal mass containing calcification (black arrow), fat (white arrow) and soft tissue components (dotted white arrow).
For this same photo without the arrows, click here
For more information, click on the link if you see this icon
Fraser and Pare
|
|
|

{kind=link}